See Explanation
[]
Gastroenterology
intestinal disorders
mesenteric ischemia
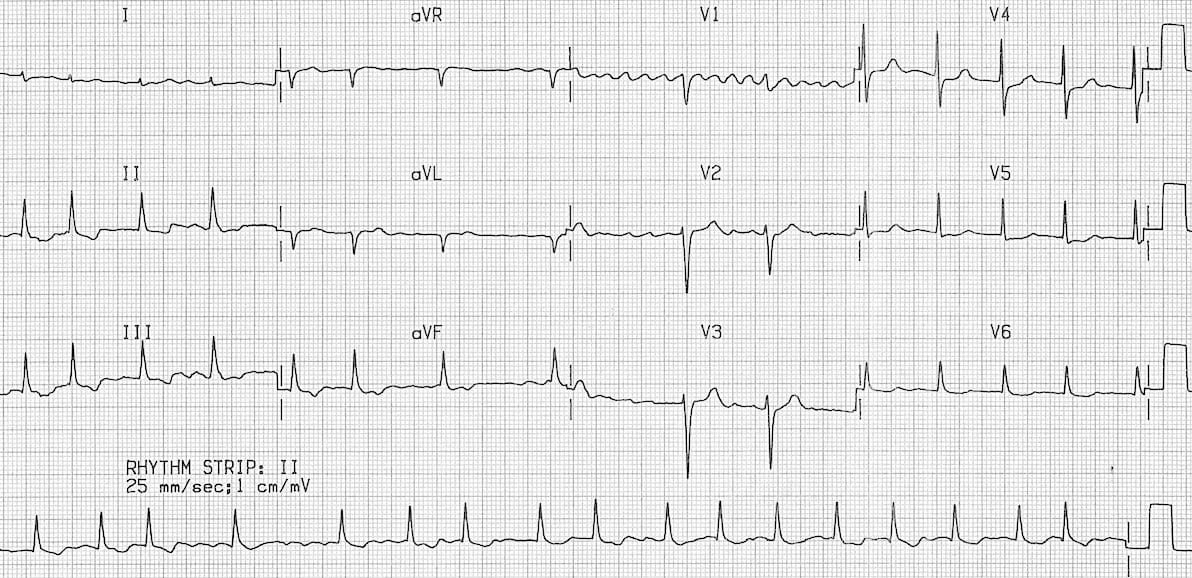
A 70-year-old man presents to the emergency department, later transferred to the medical ward, complaining of acute, severe, diffuse abdominal pain that began abruptly about 36 hours ago. He describes the pain as excruciating, disproportionate to physical findings, and initially presented with mild cramping but rapidly progressed. He reports persistent nausea, a single episode of non-bloody emesis, and melena since onset. His medical history includes hypertension, coronary artery disease, chronic obstructive pulmonary disease, type 2 diabetes mellitus, and paroxysmal atrial fibrillation for which he takes rivaroxaban. On examination, he is afebrile with a temperature of 37.1°C, blood pressure 125/75 mmHg, pulse 98/min and irregularly irregular, and respiratory rate 18/min. Cardiac auscultation reveals an irregularly irregular rhythm with no significant murmurs. Abdominal examination reveals only mild, generalized tenderness without rebound or guarding, a notable disparity with his reported pain intensity. Bowel sounds are diminished. Rectal exam confirms melena. Given this clinical picture, considering his cardiac history, what is the most likely diagnosis and what immediate therapeutic intervention should be prioritized?
| Lab Parameter | Value | Reference Range |
|---|---|---|
| Hemoglobin | 98 g/L | 130-170 g/L |
| White blood cells | 21.2 x 10^9/L | 4.0-11.0 x 10^9/L |
| Sodium (serum) | 142 mmol/L | 135-145 mmol/L |
| Chloride (serum) | 102 mmol/L | 98-106 mmol/L |
| Potassium (serum) | 4.1 mmol/L | 3.5-5.0 mmol/L |
| Bicarbonate (serum) | 18 mmol/L | 22-29 mmol/L |
| Creatinine | 105 µmol/L | 60-110 µmol/L |
| Lactate | 4.5 mmol/L | 0.5-2.2 mmol/L |
| D-dimer | 1.2 mg/L FEU | normal <0.5 mg/L FEU |
| Hemoglobin A1c | 11.8% | less than 5.7% |
Edit question